

I personally do not enjoy when strangers smile at me after checking out my bump, maybe this is why. I do however typically give an understanding smile to another pregnant woman if we cross paths.
I personally do not enjoy when strangers smile at me after checking out my bump, maybe this is why. I do however typically give an understanding smile to another pregnant woman if we cross paths.
I have been reading a very interesting and insightful book called “Waterbirth: A Midwife’s Perspective” by Susanna Napierala (1994). I will probably be posting quite a bit of information I retrieve from this book on this site because I like it so much. Anyway, the following “Pregnant Patient’s Bill of Rights” is endorsed by the International Childbirth Education Association (ICEA).
1. The Pregnant Patie4nt has the right, prior to the administration of any drug or procedure, to be informed by the health professional caring for her of any potential direct or indirect effects, risks, or hazards to herself or her unborn or newborn infant which may result from the use of a drug or procedure prescribed for or administered to her during pregnancy, labor, birth or lactation.
2. the pregnant patient has the right, prior to the proposed therapy to be informed, not only of the benefits, risks, or hazards of the proposed therapy but also of known alternative therapy, such as available childbirth education classes which could help to prepare the Pregnant Patient physically and mentally to cope with the discomfort or stress of pregnancy and the experience of childbirth, thereby reducing or eliminating her need for drugs and obstetric intervention. She should be offered such information early in her pregnancy in order that she may make a reasoned decision.
3. The Pregnant Patient has the right, prior to the administration of any drug, to be informed by the health professional who is prescribing or administering the drug to her that any drug which she receives during pregnancy, labor and birth, no matter how or when the drug is taken or administered, may adversely affect her unborn baby, directly or indirectly, and that there is no drug or chemical which has been proven safe for the unborn child.
4. The Pregnant Patient has the right if caesarean section is anticipated, to be informed prior to the administration of any drug, and preferably prior to her hospitalization, that minimizing her, and in turn, her baby’s intake of nonessential pre-operative medicine will benefit her baby.
5. The Pregnant Patient has the right, prior to the administration of a drug or procedure, to be informed of the areas of uncertainty if there is no properly controlled follow-up research which has established the safety of the drug or procedure with regard to it’s direct and/or indirect effects on the physiological, mental and neurological development of the child exposed, via the mother, to the drug or procedure during pregnancy, labor, birth, or lactation – (this would apply to virtually all drugs and the vast majority of obstetric procedures.
6. The Pregnant Patient has the right, prior to the administration of any drug, to be informed of the brand name and generic name of the drug in order that she may advise the health professional of any past adverse reaction to the drug.
7. The Pregnant Patient has the right to determine for herself, without pressure from her attendant, whether she will accept the risks inherent in the proposed therapy or refuse a drug or procedure.
8. the Pregnant Patient has the right to know the name and qualifications of the individual administering a medication or procedure to her during labor or birth.
9. The Pregnant Patient has the right to be informed, prior to the administration of any procedure, whether that procedure is being administered to her for her or her baby’s benefit (medically indicated) or as elective procedure (for convenience, teaching purposes or research).
10. the Pregnant Patient has the right to be accompanied during the stress of labor and birth by someone she cares for and to whom she looks for emotional comfort and encouragement.
11. The Pregnant Patient has the right after appropriate medical consultation to choose a position for labor and for birth which is least stressful to her baby and to herself.
12. The Obstetric Patient has the right to her baby cared for at her bedside if her baby is normal, and to feed her baby according to her baby’s needs rather than according to the hospital regimen.
13. The Obstetric Patient has the right to be informed in writing of the name of the person who actually delivered her baby and the professional qualifications of that person. This information should also be on the birth certificate.
14. The Obstetric Patient has the right to be informed if there is any known or indicated aspect of her or her baby’s care or condition which may cause her or her baby later difficulty or problems.
15. The Obstetric Patient has the right to have her and her baby’s hospital medical records complete, accurate and legible and to have their records, including Nurses’ Notes, retained by the hospital until the child reaches at least the age of majority, or, alternatively, to have the records offered to her before they are destroyed.
16. The obstetric Patient, both during and after her hospital stay, has the right to have access to her complete hospital medical records including Nurses’ Notes, and to receive a copy upon payment of a reasonable fee and without incurring the expense of retaining an attorney.After reading this in it’s entirety and having experience of having two children in two different hospitals, I would suggest that your partner also be aware of these rights and encourage both the mother and partner to ask questions as often as needed or wanted. Much of the information in this bill of rights is not often provided or offered, it is the patient’s responsibility to ask for the information.
1. Where did the midwife receive her training, and with whom did she train?
– There are differences between a Certified Nurse Midwife (CNM) and a Traditional Midwife
2. With what complications has she had hands-on experience?
– This is important because complications can arise with every birth regardless of how healthy the woman is and even with an uncomplicated pregnancy. You’ll want to know if she is experienced with emergencies.
3. At how many births has she been the primary caregiver? How many has she attended at home and how many in the hospital?
– And how did those births go?
4. What is her philosophy about pregnancy and birth?
5. Will she be an active participant in the prenatal care? and postnatal care?
6. Does she have doctor backup for consulting? Does she have a doctor who will meet the mother and her at the hospital if any complications occur during labor?
7. If no doctor backup is available, what plan of action does she have in case of an emergency?
8. How soon does she go “on call” before the baby is due?
9. When does she come to the birth?
10. Will she bring an assistant? and how many?
11. What equipment does she bring to the birth?
12. How long does she stay after the birth?
13. When does the midwife start her postpartum care?
14. What are her fees? Do her fees include payment for the assistant? and what other costs are involved?
15. Most importantly ask yourself: How comfortable am I with this person and do I trust her training and instincts.
Retrieved information from: Waterbirth: A Midwife’s Perspective. (1994) by Susanna Napierala.
I was searching videos of home water births on Youtube and found a few that I would like to share.
The first is “Oliver’s Gentle Waterbirth” using Hypnobirthing as a method of relaxation. Here is the link:
The second is a “Surprise Twin Homebirth”. This one scared me a little because everyone says Im having multiples which I really believe is not true due to having an ultrasound but here is the link:
The third is “Taylor’s Natural Breech Birth”. I think it looks a little too easy compared to what I’ve heard about breech birth being more difficult but maybe I didn’t see her anguish…here is the link:
The fourth is “Sadie’s Natural Home Waterbirth”. Here is the link:
Two More…
The fifth is “The Home Birth of Lemma Maria” and here is that link:
And the sixth is “Natural Birth Encouragement – Pain and Joy” and here is the link to that one:
Now, the headline might confuse some people. What do you mean considering? Isn’t that a regulated, mandatory test? The answer is “No”. Many women or couples do not question their doctors when they are told, “It’s time for the Group B Strep Test” and they follow directions to have it done. That’s not really that big of a deal but most people are not told that the test is optional. They are also not told that if you choose to take the test, the doctor will insist that you treat Group B Strep with at least 2 rounds of antibiotics while you are in labor. The antibiotics are usually given at 4 hour intervals which basically sets the stage for being in the hospital for minimally 8+ hours in labor. Once your contractions start regularly and they can justify keeping you, you better believe they will want to start those antibiotics.
Im providing this information for several reasons. I have first hand experience with the above situation. I was taught that doctors are “all knowing” and should be shown reverence. Doctors are people with training and have a set of beliefs that may or may not be similar to your own so I always encourage people to ask as many questions about instructions that they are given. I have also tested positive twice for Group B Strep. With my first, I ended up having antibiotics. It was my first child, I had no idea what I was doing even though I read every book I was handed regarding childbirth. With my second, my doctor recommended that I get tested due to my prior history with the bacteria. She knew that I did not want treatment with antibiotics before she recommended this but did not tell me that if I tested positive, which I did, I would be pressured to have the antibiotics. This whole issue strained my relationship with my doctor and due to several other reasons, I hired a different doctor at 37 weeks pregnant. Luckily…I think, my second child was in a hurry to enter the world after 6 days past her expected date of arrival. We were only in the hospital for maybe 20 minutes before she was born. Needless to say, I did not have antibiotics with her birth and my sweet little girl is very healthy and never had any complications. I also did extensive research during this time to learn more about the bacteria and the complications it could cause.
Group B Strep (GBS) is a type of bacteria found in the vagina and/or lower intestine of 10-35% of all healthy adult women. Most of the time, the bacteria lives in balance with other bacteria and is considered normal, but there are instances when the bacteria does not live in harmony with other bacterias and could travel to other parts of the body such as blood stream, urinary tract, or the meninges which could cause some problems.
Pregnant women testing positive for GBS could develop urinary tract infections, amnionitis, or endometritis. Amnionitis could cause the menbranes to rupture prematurely, resulting in a preterm or stillbirth. In most cases, women remain asymptomatic and are only carriers of the bacteria.
So, how does this affect the baby if the mother is a carrier? If the mother has a long pushing time, or if the woman’s water breaks and there is a long time before delivery, there is a higher chance that the baby could be affected by Group B Strep. The baby would contact the bacteria as he/she passes through the birth canal if the membranes rupture and the bacteria enters into the amniotic fluid. When considering this process, it seems very low risk, right? Well yes, because most babies who are exposed to the bacteria have no symptoms and do not contract any illness. There is a small percentage of babies that do which poses the concern. The illness is called Early Neonatal Group B Streptococcal Septicemia (ENGBSS). The GBS infects the bloodstream and coupld potentially spread to the meninges (water which surrounds and protects the brain) resulting in meningitis. Scary right? Yes but the percentage is very low. Most cases of GBS infections are early on-set which occurs in the first week of life with more than 90% manifesting in the first 24 hours. There is also a late-onset illness which occurs between ages 1 week and 3 months old.
Signs and symptoms of babies who may be affected: temperature instability, breathing problems, grunting sounds, cyanosis, fever, seizures, stiffness, or lethargy. These are not normal symptoms for healthy babies so you would want this monitored and treated if you notice theses signs.
So here are the stats. Each year there are approximately 8000 babies in the U.S. who contract serious GBS disease and of these 10% will be fatal or 800 babies. Another source states that 300 babies die each year from GBS disease. The Center for Disease Control estimate the risk of a baby contracting GBS disease is .5/1000 births. All sources agree that it is a very small number of babies affected, strict protocols are in affect written by the CDC which mandates doctors to insist on every women being tested. Precursors to insistence on antibiotics include: Previous baby with GBS sepsis, regardless of current colonization, preterm labor (less than 37 weeks), ruptured membranes for more than 18 hours, intrapartum temperature greater than 100.4, GBS found in urine.
Issues with the protocol are that the colonization of the bacteria is taken at approximately 36 weeks gestation. The bacteria colonization can come and go within days. With that being said, a woman can test positive for GBS at 36 weeks but actually have no evident bacteria at the time of labor, or vice versa. This protocol has lead 1/3 of all pregnant women and their babies to be treated with I.V. antibiotic during labor. This has also caused an increase is antibiotic resistant bacteria, not just in GBS strains but in other bacteria such as E coli. A study of 43 infants with blood infections caused by GBS and other bacteria found that when the mother was treated during labor with I.V. antibiotics, 88-91% of the infants’ infections were resistant to antibiotic treatment. In mothers not treated during labor, 18-20% of the infections were resistant.
Alternative protocols do exist!!! Yay! I never knew this until just now but there are herbal therapies which unfortunately have not be scientifically proven but have been effective. Here they are”
* Garlic (natural antibiotic) – 1 clove daily either orally or vaginal suppository
*Echinacea Root Tincture – 1 time daily
*Vitamin C with Bioflavonoids (helps strengthen the amniotic sac)- 1,000ml daily
*Probiotics (adds good bacteria to balance system) – as directed
Another safe alternative treatment that is recommended by my midwife is rinsing the vaginal and rectal areas with Hibiclens every 4-6 hours during labor, after the membranes have ruptured. Hibiclens is a brand name for chlorohexidine, an antiseptic solution that is safe for both mother and baby yet very effective in reducing the incidence of GBS and E coli infection in newborns. There have been specific scientific studies done which have proven the effectiveness of this treatment (J Matern Fetal Neonatal Med 2002 Feb; 11(2);84-8 and British Journal of Medicine 1997 Jul 26;3 15 (7102);216-9).
Much of this information was provided by Blessings of the Womb Midwifery Services, Robin Lavis, CPM. I do have more articles that I will eventually add to this topic regarding GBS but unfortunately were not in the piles of information that I thought it was in. Stay tuned.
Although I have tested positive in both my other pregnancies and had two very different experiences, both with healthy babies, I will be opting out of this test. I do plan to use the Hibiclens as well as the herbal protocols to ensure a healthy birth. My decision is also based on the fact that I have done extensive research and I have very short labors and my water has not broken up until the very end stage of labor in the past.
As always, please do your research before making any health decisions that affect you or your loved ones. There are very good reasons for recommendations regarding illness but you must be an informed decision maker in your healthcare to be effective in staying healthy.
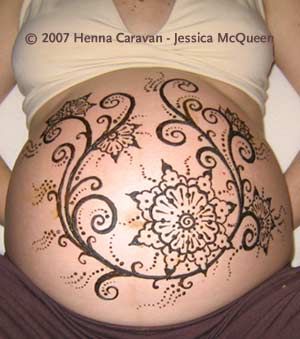
During my last pregnancy I was able to hire someone locally to do henna art on my belly and it was a very cool experience. I thought my second child was going to be my last so I pretty much did most of the things I wanted to do and this was one of them. The local Artist is Martina Hahn and her contact information is as follows: Moments in Time Art Studio 231-675-7071 located in Boyne City/Walloon Lake area. Website: http://www.m-Art-ina.com
The following photo is what Martina did for me: 
And here are some really cool designs. I found them on Pinterest along with a slew of others: 





A family member of mine has asked me about increasing milk supply. I will probably be posting more articles on breastfeeding once I find them and for now I would like to share this photo of foods that are known to increase the milk supply. I always suggest discussing your troubles with a lactation consultant or midwife or doctor in case there are other factors. The best advice I usually give with specifics is to make sure you are drinking lots of water to stay hydrated, eat enough calories to support the food supply, skin to skin contact, and pumping between feedings. Stay tuned for more…
This is another gem from my birthing classes that I thought I would share as good information:
Physiological:
Mom:
Baby:
Emotional:
Practical:
Function:
Learned skill:
Positioning:
How often? How long?
Supply
To increase milk supply (will increase in 48 hours)
Problems:
Sexuality:
Bottle Feeding:
Mom:
Baby:
Now, I realize there may be some criticisms regarding this information however this is provided to point out the benefits of breastfeeding. Understandably some people will choose formula over breastfeeding, however, I will continue providing information that I believe is most beneficial to mom and baby throughout this blog.
One of the most frustrating things that I hear from women is that they do not have enough milk for their baby. Our body is designed to produce milk for our littles and if we take proper care of ourselves then we should be able to produce milk. I encourage all women who are concerned about their milk supply to reach out to a lactation consultant or midwife, possibly even a doctor or nurse with your concerns in order to try changing something in your life that my make a huge difference for your baby’s nutrition.
The information I am providing today comes from my midwife: Robin Lavis of Blessings of the Womb in Rapid City, MI. I completed her birthing classes and this is some of the information she taught us. I thought it was pretty ingenious to use this method since I have spent what seems like an enormous amount of time pumping and storing breast milk from my first two children. I would store it in the bottles until I got home and then I would measure certain amount of ounces depending on the baby’s age and labeling…ugh…seems ridiculous now but I thought I was doing the best I could to preserve my supply and use wisely. So, to fill you in…this is the information below:
“If you find that you must return to work after the birth, please know that it is still possible to continue breastfeeding your baby. Many women find they can manually express milk easily and do not need a pump. Others still prefer using a pump. You can either buy or rent a good breast pump for an affordable price. I recommend the Medela Breast pumps (So do I). Every model is excellent but the double electric is what you need if you are returning to work full-time. Women generally have the greatest milk supply in the morning and find it is a convenient time to pump. If you must pump while you are away from your baby, bring a photo of your baby along with you to help get the milk flowing. One of the easiest ways to collect breast milk is while the baby is nursing you can use a ‘Milk Saver’ on the other breast.
Using ice cube trays to freeze the milk and then immediately transferring them to a glass jar is a convenient and safe way to store your breast milk. It keeps the milk away from freezing in plastics and every ice cube (in a 14 cube tray) is one ounce of milk. You can store breast milk in the freezer for 6 months in a two door fridge/freezer, 2 weeks in a 1 door fridge/freezer and 1 year in a deep freeze. Refrigerate milk if you plan to use it within 24 hours. Remember to put a date on the stored breast milk.”
I love this idea! Im planning to buy a lot of mason jars 🙂 Here is the link to what a Milk Saver is: http://www.mymilkies.com/milksaver
I want to apologize for my recent lack of posts. I started this blog to begin my journey providing services to those who want to become pregnant, are pregnant, or have recently had a baby in order to provide support for those who want or wanted natural birthing experiences. Well, I realized I was completely miserable working in my previous job for many reasons and decided to make a career change. Part of this blog was to enter my own counseling/advocacy services but I couldn’t wait to build my business slowly and decided to take a job working as a Hospice Social Worker. I am finally in my comfort zone with this new position and while they expect to give me more responsibilities soon, I do want to make this business a priority. I plan to be more active in posting more resources and services as well as helpful articles but I am estimating January as my more productive month once the holidays are behind us. If anyone is interested in services please do not hesitate to contact me. I can also help to find you resources in Northern Michigan if you are looking or curious.
